Dental Implants
Our teeth are an important factor in various functionalities, including talking and chewing, as well as aesthetics. The crown, which is the visible part of the tooth, is covered by hard enamel that is able to withstand the pressure of chewing and tearing food. The root of the tooth is composed of dentin. It is embedded in the jawbone and is normally not visible. The bone that envelopes the roots of the teeth is what holds them in place.
Sometimes, as part of an overall treatment plan, teeth need to be extracted. There are many reasons for extracting teeth, including crowded dentitions, various pathological processes, and infections in parts of the teeth and the surrounding tissue.
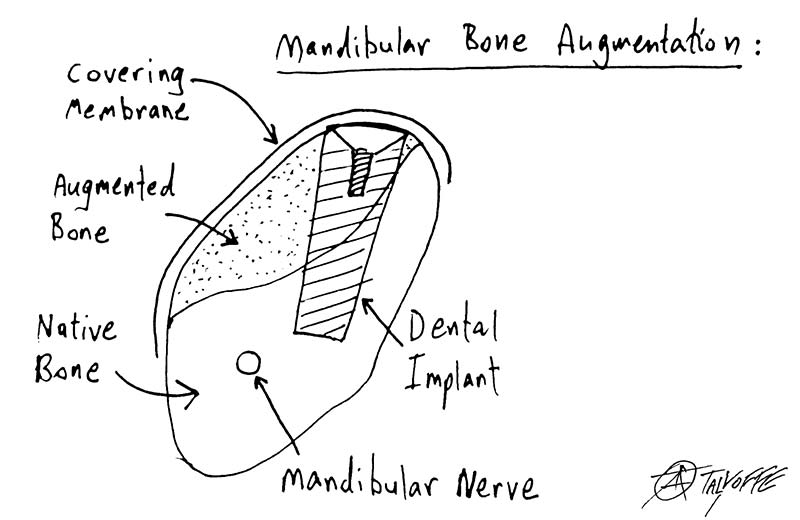
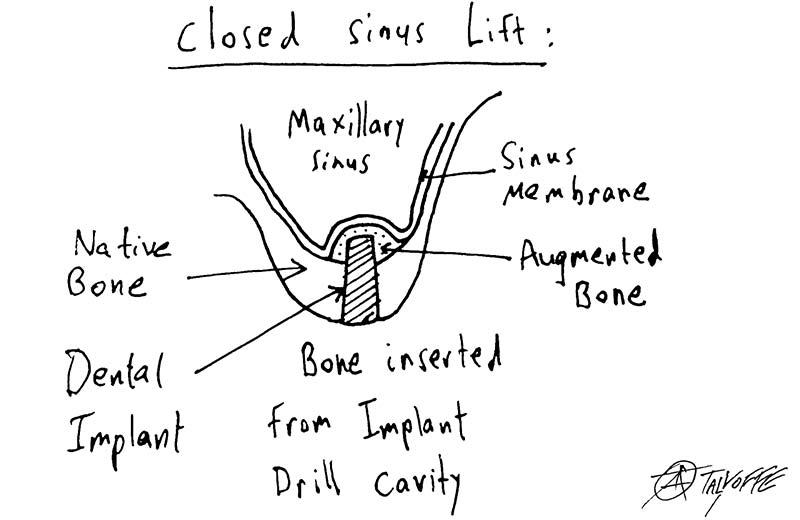
Dental implants replace the roots of the tooth and are inserted into the jawbone where the teeth were extracted. The implants can be placed immediately after extracting the tooth, but usually, due to the amount and quality of the bone it can only be done several months later. Sometimes, when the tooth is extracted, the jawbone, which has been damaged by the same causes that necessitated the extraction, needs to be augmented in order to preserve the alveolar volume. After placing the implants in the jawbone and waiting several months for the bone to heal, giving the implants stability and the ability to withstand the strain, the prosthodontist (oral rehabilitation doctor) can build the crowns on top of the implants. Cooperation between the surgeon and the prosthodontist is crucial to the success of the entire treatment. In special cases, the crowns can be positioned on the same day the implants are inserted. Determining the location of the implants, their dimensions and the distribution of force they will need to withstand, while taking into account the patients' desires and abilities, is challenging and requires meticulous planning, using advanced technologies, such as 3D models, and vast professional experience.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Surgical Extraction of Impacted Teeth
There are many reasons to extract teeth, including caries, gum problems, infections, crowded dentitions, supernumerary (redundant) teeth and impacted teeth.
Teeth that are fully impacted often do not need to be extracted. However, sometimes their presence can cause complications. For example, the dental sac that surrounds the crowns of the impacted teeth can enlarge and develop into a cyst that grows in a way that harms the jawbone and makes it thin and prone to fracture.
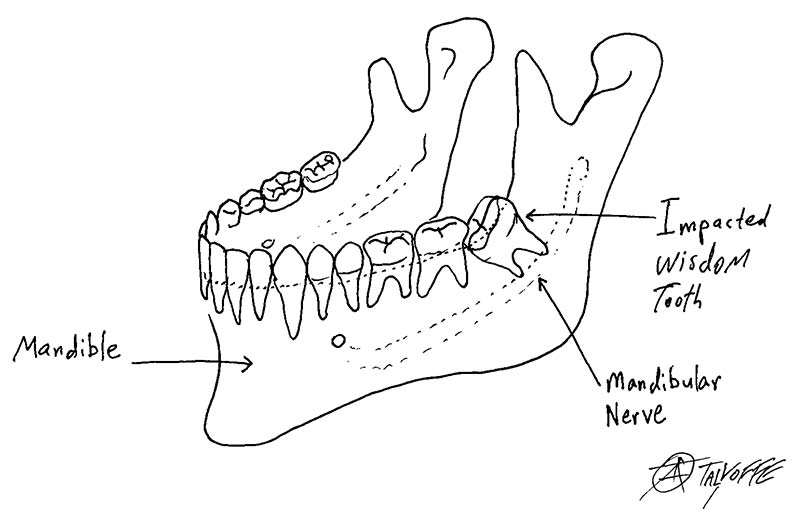
In addition, the presence of impacted or redundant teeth could interfere in orthodontic procedures. Partially impacted teeth are likely to cause more trouble than fully impacted teeth. Their partial impacted position means that the crown is exposed in the oral cavity, like the tip of an iceberg. The gums can grip the neck of the tooth, which is the part of the tooth between the crown and the root and is not coated by enamel, but cannot grip the enamel that covers the crown of the tooth, which is exposed to the oral cavity. This creates a pocket through which bacteria can penetrate the length of the tooth, causing chronic infection, which can lead to pain, damage to nearby teeth, swelling and unpleasant odours. The most common impacted teeth are wisdom teeth and canines. However, impacted and supernumerary teeth can occur in any jaw and anywhere teeth sprout.
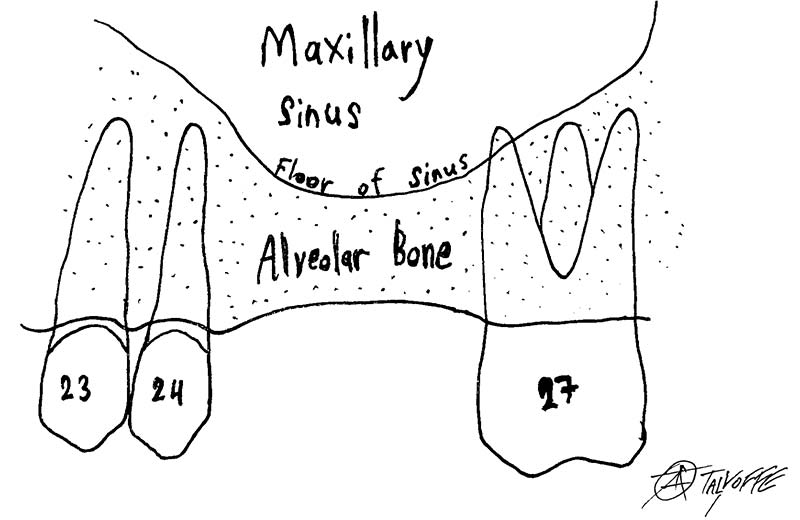
Sometimes, impacted teeth are very close to important anatomical structures such as the lingual nerve, mandibular nerve or the maxillary sinus. In such cases, it is important to consult an oral and cranio-maxillofacial surgery specialist. Surgical extractions do not usually need to be performed in a hospital.
Exposing Impacted Teeth for Orthodontic Treatment
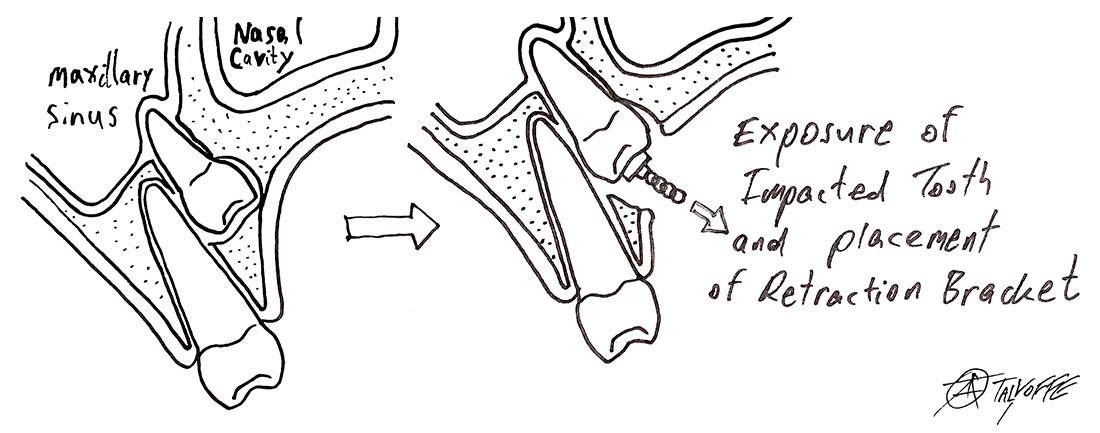
As part of an orthodontic treatment, sometimes impacted teeth need to be exposed to help them erupt into place. The teeth that need to be pulled into place could be impacted deep in the jaw, and exposing them requires skill and experience.
After exposing the impacted tooth, a bracket is bonded to its crown. A chain attached to the bracket is used to pull the tooth into the right direction until it reaches its proper place in the oral cavity.
Biopsies of Soft and Hard Tissue in the Oral Cavity and the Face
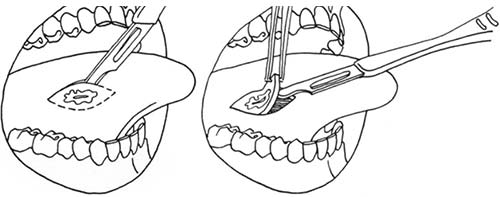
When tissue in the face or the oral cavity is identified as being superfluous or out of place, has a different composition or looks abnormal; when a lesion does not heal or improve within a few days; or when imaging findings are suspicious; diagnostic surgery should be considered.
This procedure is called a biopsy. The word biopsy derives from the Greek bio, meaning life, and opsis, which means sight.
Head and neck cancer is the seventh most common type of cancer, and is affected by several risk factors, including smoking, alcohol consumption, bad oral hygiene, genetic predisposition and various viruses (HPV, EBV).
It is important to have an oral and maxillofacial surgeon periodically examine the mucous membranes of the oral cavity once you reach the age of 40.
If a biopsy has been taken, the sample will be examined under the microscope for diagnosis. Sometimes, treatment ends with the biopsy and no further steps are needed, and sometimes the biopsy is only the first step.

Surgical Treatment of Patients with Complex Medical Backgrounds
An important preliminary stage of any medical treatment in general and surgical procedures in particular is obtaining a thorough anamnesis (medical history) and understanding the full medical background of the patient, including their habits, medications, sensitivity to certain substances or drugs, past hospitalizations and previous surgical procedures.
Some background information will require special attention, such as cardiac or pulmonary conditions, oncological pasts, having received direct radiation to the head and neck area, imbalanced diabetes, poor renal function, and taking anticoagulants or platelet-aggregation inhibitors, drugs that interfere with the immunological response, or drugs that can delay or impact bone healing and remodelling, to name a few.
The older the patient is, the more likely they are to have one or more of these conditions, and a broad medical perspective is needed in order to suit the right treatment to the patient.

Treating Patients with problems in the Joints and Muscles of the Masticatory (Chewing) System
The lower jaw, the mandible, is classified as a long bone. Its frontal part, the body of the mandible, is shaped like a horseshoe that crosses the midline, and it holds the teeth. The two back parts—one on each side of the face—have perpendicular structures that end in ball-and-socket joints at the base of the skull, which are called the temporomandibular joints (TMJs). Each of these TMJs is a complex anatomical structure containing a cartilage disc located between the ball and the socket that is surrounded by a system of tendons, ligaments and muscles responsible for stabilizing and moving the mandible.
Surgical Procedures Using “Laughing Gas” (Nitrous Oxide), General Anaesthesia and Sedation
When a patient suffers severe anxiety before a surgical procedure, or when full cooperation of the patient throughout the treatment cannot be guaranteed (for example, with children who need dental treatment), there are several methods that can be used to help complete the procedure:
Using laughing gas - A mixture of oxygen and nitrous oxide is inhaled through the nose and carefully monitored by the doctor. Special training is required before a dentist may administer nitrous oxide, and not every dentist is licensed to use it. Using nitrous oxide on pregnant women is prohibited. Laughing gas has practically no side effects, although patients might temporarily feel a little dizzy or nauseous after using it.
General anaesthesia and sedation - Technological advances and improved skills, combined with a rise in the demand to carry out several procedures at once, have also brought about an increase in using these methods. However, we must remember that they are not risk free. Using anaesthesia and sedation require the presence of an anaesthesiologist and a dentist with a special license from the Ministry of Health.